
Recent U.S.-African Health Agreements Face Backlash

President Donald Trump greets Democratic Republic of the Congo President Felix Tshisekedi at the U.S. Institute of Peace, Dec. 4, 2025, in Washington. (AP Photo/Evan Vucci, File)
In Sept. 2025, the U.S. released the America First Global Health Strategy, focusing on American-funded health assistance programs run bilaterally globally, focusing on Sub-Saharan Africa. The U.S. has signed 24 Memorandums of Understanding (MOUs) — 20 with African nations. Amongst the nations involved are Nigeria, Kenya & Rwanda — three big players paving Africa’s health landscape. By focusing on direct government funding, the deals made by the U.S. total approximately $19 billion over the next five years. This funding is tied to much-needed support for diseases such as HIV, malaria, tuberculosis and other major health threats that cripple densely populated countries in Sub-Saharan Africa. As conditions of these deals, the U.S. required an increase in domestic healthcare expenditure and a disclosure of valuable pathogen data. These deals have been framed by the U.S. as methods of reducing future aid-dependency and bolstering healthcare systems in Africa.
Pathogen-sharing is important and has profound value to the U.S. government as African nations have much more lenient procedures when testing/experimenting with diseases on the population. The U.S. constitution prevents any legal form of testing on patients through restrictive FDA regulations and the Common Rule on human testing research. A precedent for this data sharing already exists. In 2021, South Africa identified and shared the Omicron variant to the global health industry through WHO channels, enabling global vaccine alterations. South Africa was slapped with harsh international travel bans that put its economy in an impaired position. The current US bilateral model demands the same data sharing but does not have a meditating third-party to ensure that drugs and vaccines return to the country providing the data.
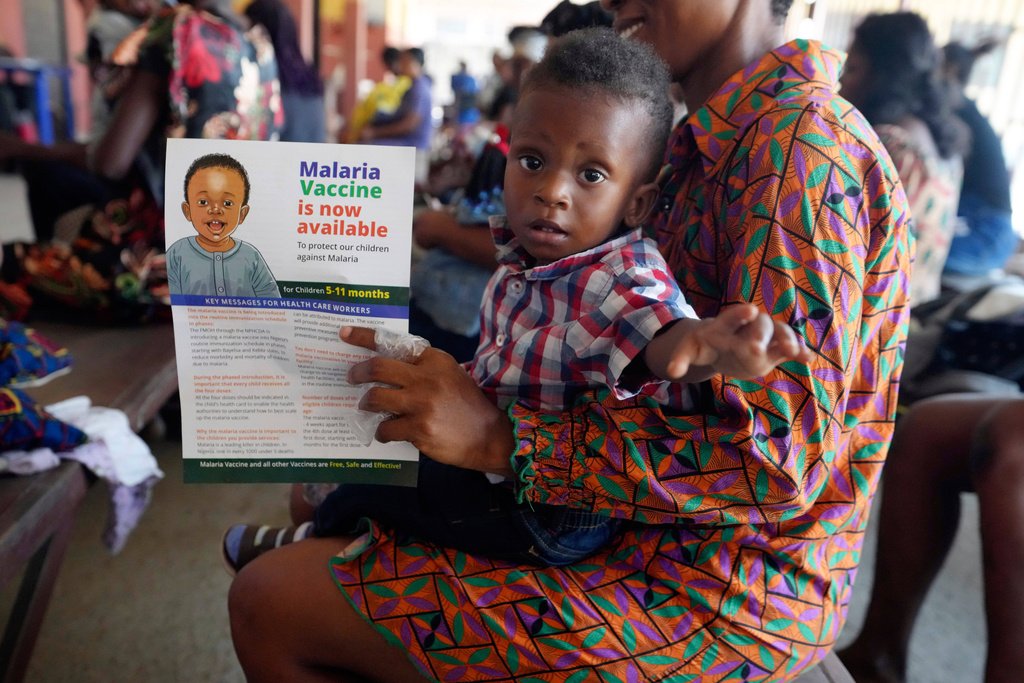
A woman waits to have the malaria vaccine R21/Matrix-M administered to her child at the comprehensive Health Centre in Agudama-Epie, in Yenagoa, Nigeria, Monday, Dec. 9, 2024. (AP Photo/Sunday Alamba, File)
On 25 Feb, 2026, Zimbabwe rejected further talks for a $367 million bilateral deal with Washington for future aid — and to fight fatal diseases with American-funded capital. Zimbabwe’s president affirmed that the national healthcare system could and would support itself going forward. This exit raises questions of potential uneasiness spreading amongst African nations in light of the Administration's requests. A U.S.-Zimbabwe relationship has lasted for 45 years but suffered a major blow from Trump’s USAID cuts in Jan. 2025, affecting Zimbabwe majorly through a loss of $522 million in funding. Zimbabwe’s reasoning, however, goes deeper: government spokesperson Nick Mangwana called the deal as “asymmetrical” and one-sided. This response comes from the U.S.’ demand for data and pathogen-sharing with no contingency that the affected African countries would eventually recieve benifits down the line. Zambia, another nation facing similar socio-economic issues, refused a $1 billion USAID health deal on the same day as Zimbabwe’s exit, for concerns regarding data sharing. Secretary Rubio’s State Department also conditioned Zambia’s cobalt and copper mining sectors as part of the deal, which raised serious concerns about the U.S.’ true motives behind the deal. All 20 health deals providing research on pathogens included a required co-investment from the host nation, as is the case with Congo which signed a $300 million investment in the healthcare industry. With such heavy investment, the functions and abilities of the national budget tighten as more resources are poured into the healthcare industry leaving other crucial funds to potentially dry up. Congo’s annual health funding gap is $1.8 billion. This model gives them $180 million per year, but binds them to pay $60 million per year, which they strategically cannot afford.
Over the last two weeks, the situation has been dynamic and evolving with four new countries signing up and more expected to join. However as seen with the cases of Zimbabwe and Zambia there is also growing backlash to the terms of these agreements. This sparks a controversial debate: Is the current U.S. Administration focused on African healthcare needs or seemingly an “America First” motif?